Research and Design Thinking in Healthcare
- Gianna M
- Dec 15, 2023
- 4 min read

Updated: Jan 7, 2025
Over ten weeks, I conducted research to examine a problem in the healthcare industry and brainstorm possible solutions. This project was completed in collaboration with an industry expert from the Penn Medicine Center for Health Care Innovation. While the proposed solution can stand on its own, I formulated it based on my understanding of the dynamics within the Penn Medicine organization.

Keep reading to learn about how I leveraged research to inform the proposed solution.
The Problem
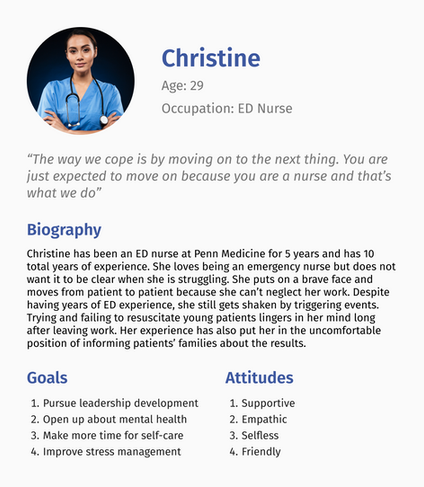
The scope of the project was to examine a problem facing healthcare professionals. I was interested in the psychological challenges and mental health concerns affiliated with healthcare professionals in high-stress environments. Through preliminary research, I narrowed my scope to emergency department (ED) nurses. I learned that these nurses may experience trauma from witnessing traumatic events, being directly involved in such incidents, or feeling burdened by their work environment.
My research led me to focus on a specific timeframe: the post-traumatic period following a critical incident (CI). While many existing measures aim to mitigate trauma before a critical incident occurs, I was more concerned with how hospital systems address lingering trauma afterward. I further narrowed my focus to emergency department nurses coping with trauma after witnessing—rather than directly experiencing—traumatic events.

Research Findings: Exploring STS
A notable constraint of this project was the lack of direct access to potential end users, leading me to rely more on online research. This constraint allowed me to grow by pushing me to adopt a problem solving approach focused on consulting existing academic sources rather than solely depending on user participation.
“Secondary PTSD, also known as secondary trauma stress (STS), is when someone witnesses a traumatic event and it indirectly affects them” (Kahrs, 2019, p. 7)
Key Takeaway: Nurses in emergency departments have constant exposure to critical incidents (e.g., failed resuscitation, car accident victims) and may experience symptoms of traumatic stress within a week of such incidents.

From analyzing direct quotes from ED nurses, I identified four possible reasons for the lasting traumatic effects of witnessing critical incidents:
Difficulty discussing trauma with higher-ranking individuals in the organization
Expectation to quickly move on after a traumatic event
Limited or no time to pause and process experiences
Lack of routine debriefing practices

Effectiveness of Existing Measures
Critical incident stress debriefing: Results are mixed. While one study found CISD reduced stress in ED nurses, others suggested it might trigger prolonged traumatic responses or even PTSD.
Personal Reflective Debriefing: This approach showed a decrease in secondary traumatic stress (STS) symptoms. Overall, debriefing is a commonly proposed solution to reduce trauma in emergency departments.
Key takeaway: Implementing personal reflective debriefing and/or critical incident stress debriefing can foster a supportive culture, reduce absenteeism, lower staff turnover, and increase job satisfaction and productivity.




Real-World Application: Insights into Penn Medicine
A brief interview with an expert from the Penn Medicine Center for Health Care Innovation provided valuable insights into the organization’s operations and the challenges that nurses face.
Key Takeaways:
Lack of a system-wide approach
Strong sense of camaraderie among nurses
Existing balance between clinical work and professional development pathways

Idea Generation
With a clear understanding of the problem and Penn Medicine’s organizational dynamics, I brainstormed potential solutions. These included discussion-based initiatives, designated hospital areas, and an uplifting bulletin board. Ultimately, I landed on the Peer Trauma Buddy program as the best fit because it allows for professional development and would therefore be easily adapted into Penn Medicine's existing professional development pathways.

With a solid understanding of the professional benefits of a Peer Trauma Buddy program, I leveraged my user experience background to ensure that my idea was also meeting the needs of the target individuals. This allowed me to identify relevant goals that I might be able to address in my solution.



Proposal: Peer Trauma Buddy Program
The Peer Trauma Buddy program proposal leverages Penn Medicine’s strengths in fostering nurse camaraderie and professional development to support ED nurses experiencing secondary traumatic stress.
How it works:
Nurses facing secondary traumatic stress are paired with a designated peer for immediate post-traumatic conversations and ongoing support
Nurses interested in career growth build leadership skills, earn certifications, and gain visibility in the organization
Next steps:
Assess ED staff interest in becoming certified peer trauma buddies or participating in the program
Develop a list of incentives to encourage participation in the program
Identify valuable resources for a self-care toolkit
With enough interest, design a pilot program
Conclusion
This project emphasized the importance of research in thoroughly understanding a problem. It also allowed me to focus on how I might combine this knowledge with empathy to propose a feasible solution that could genuinely improve lives. While the Peer Trauma Buddy program remains a concept, it is something I would be thrilled to see implemented in a real-world setting.
Bibliography
Davis, R. (2020). Critical Incident Stress Debriefing for Nurses in Emergency and Critical
Care Departments. MSN Capstone Projects. http://hdl.handle.net/10950/2603
Kahrs, R. (2019). Debriefing After Traumatic Events for Emergency Nurses: A Way to
Decrease Secondary Traumatic Stress.
Lavoie, S., Talbot, L. R., & Mathieu, L. (2011). Post-traumatic stress disorder symptoms
among emergency nurses: their perspective and a “tailor-made” solution. Journal of
Advanced Nursing, 67(7), 1514–1522. https://doi.org/10.1111/j.1365-2648.2010.05584.x
Magyar, J., & Theophilos, T. (2010). Review article: Debriefing critical incidents in the
emergency department. Emergency Medicine Australasia, 22(6), 499–506. https://doi.org/10.1111/j.1742- 6723.2010.01345.x
Morrison, L. E., & Joy, J. P. (2016). Secondary traumatic stress in the emergency
department. Journal of Advanced Nursing, 72(11), 2894–2906. https://doi.org/10.1111/jan.13030
Nieves, A. (2019). Factors Contributing To The Negative And Unhealthy Psychological
Conditions In The ED RN. https://stars.library.ucf.edu/honorstheses/462
Comments